A picture archiving and communication system (PACS) is a computerised means of replacing the roles of conventional radiological film: images are acquired, stored, transmitted, and displayed digitally. When such a system is installed throughout the hospital, a filmless clinical environment results. Although there are many hundreds of PACS installations operating throughout the world, many are only small, linking, for example, the intensive care unit with the radiology department, or networking a few workstations together, and it is questionable whether such systems merit being described as a PACS. There are still relatively few (less than 20) truly filmless hospitals in existence.1 ,2
The advantages of PACS
Were the replacement of conventional xray film the only role of PACS, then it would be an unjustifiably expensive and highly complex way of achieving this goal. The main advantage a PACS offers is the improvement in efficiency resulting from electronic data handling:
- Once an image has been acquired onto PACS it cannot be lost, stolen, or misfiled. (Many hospitals report that 20% of films are missing when required, creating a serious practical problem.) Thus, images are always available after a PACS has been installed, so no patient appointment is cancelled, no clinical decision deferred, no images are repeated because they are missing, and no time is wasted by doctors or other healthcare workers looking for missing films. All images are available day and night for viewing anywhere in the hospital (and outside the hospital if there is a teleradiology facility).
- The numerous PACS terminals throughout the hospital allow simultaneous multilocation viewing of the same image, if desired, whereas conventional film can only physically exist in one place at any one time. This means, for example, that a doctor in the accident and emergency department can discuss a patient’s images with the radiologist, with both clinicians viewing the images yet neither having left their department. Similarly, by the time a patient has returned to the outpatient department after being sent for an urgent radiological examination, the images will be available on PACS for viewing by the referring doctor.
- The PACS database ensures that all images are automatically grouped into the correct examination, are chronologically ordered, correctly orientated and labelled, and can be easily retrieved using a variety of criteria (for example, name, hospital number, date, referring clinician, etc). All imaging studies of a patient are immediately available on the PACS which encourages review of examinations with preceding studies and intermodality comparisons. Although difficult to prove, this would clearly be expected to be clinically beneficial.
- Working with soft copy images on monitors allows the full gamut of computer tools to be used to manipulate and post-process the images (fig 1). Alteration of the contrast width and level allows soft tissue and bony structures to be well seen on a single exposure. For example, it often permits the left lower lobe to be assessed behind the left cardiac silhouette, whereas this information is not available on a relatively under exposed hard copy chest radiograph (fig 2). There is thus an increase in the amount of information which can be extracted from an image, which is particularly noticeable for plain radiography. This is also partly the result of the photostimulable phosphor plate acquisition device generally used for acquiring these images in a digital format. These phosphor plates have a greater dynamic range than the conventional screen–film combination which leads to improved simultaneous visualisation of structures of widely differing radiodensity, and also permits a lower exposure dose to be used in many cases (fig 3).
- PACS does allow some direct economic savings from the lack of expenditure on film, film packets, film processing chemicals, staff salary savings from darkroom technicians, and film filing clerks, and the redeployment of space previously used for film storage. Cost savings are, however, not as great as predicted, because although dark room technicians are no longer needed, they are replaced by fewer, higher paid information technology managers and other computer personnel. The aim when introducing a PACS is to be at least cost neutral with respect to conventional radiology. If economic savings are made, this is a bonus. The real advantage of a hospital wide PACS is the huge increase in efficiency of data management it provides.

{kind=link}
{kind=link}
Figure 1
Example of PACS computer tool: linear measurement of cardiothoracic ratio drawn onto soft copy chest image.

{kind=link}
{kind=link}
Figure 2
(A) Digitally acquired soft copy chest image with greyscale window width and level set to give good penetration of the left lower lobe through the cardiac silhouette. (B) Same image windowed to simulate an under exposed chest image showing superficial soft tissues, but suboptimally showing structures behind the heart.

{kind=link}
{kind=link}
Figure 3
Graph showing the sigmoid relation between optical density and radiation exposure for conventional film–screen radiography, compared with the linear response seen with photostimulable phosphor plate computed radiography. The phosphor plate has a much greater dynamic range (latitude) falling within diagnostic levels of optical density, and so can show a larger number of tissue structures well at any given exposure, and responds better than film at lower doses.
The Hammersmith Hospital PACS: background
The Hammersmith Hospital in West London has been operating as a totally filmless hospital since March 1996.3 Films are printed only for use at outside institutions. There is a centralised storage system with a long term archive of 2 terabytes on optical disks (with plain radiographic images lossily compressed after reporting at 10:1), and a short term storage system of approximately 10 days worth of imaging examinations on a 256 gigabyte random array of inexpensive disks (RAID) (fig 4). (A RAID is a multitude of hard drives (or disks) where the information is written to all the disks so that it is distributed over the entire RAID. This means that if any of the disks were to fail, only a small proportion of the data would be lost. In addition, the RAID management software has an error correcting algorithm which is able to rewrite any lost data with a high degree of accuracy, so that data loss is very unlikely.) The network architecture of the PACS is centralised, with the archives at the hub and the 168 workstations and 23 imaging modalities on spokes, each connected to the hub by a dedicated point to point high capacity optical fibre using a fast protocol, as rapid transmission is crucial for moving around the vast amount of data contained in radiological images. (There are approximately 10 megabytes of data in one chest radiograph.) Textual demographic data are carried by slower ethernet protocol.

{kind=link}
{kind=link}
Figure 4
Diagram of the centralised Hammersmith PACS architecture.
Images are retrieved in two seconds from short term storage and in approximately two minutes from long term storage. The vast majority of images viewed in the hospital are already on the short term server as they have been prefetched overnight prior to being needed the following day. Integration of the PACS with the hospital and radiological information systems (HIS and RIS) triggers the appropriate prefetches as these latter systems know which patients will be in- or outpatients the following day, and which have been booked to undergo imaging procedures.
When the PACS was implemented at Hammersmith, the various clinical disciplines were brought “on line” sequentially (rather than all at once) in order to be able to concentrate technical and training resources on those areas which were “going live”. Paediatrics and the neonatal unit (NNU) were among the first clinical specialties to start using the PACS, because these specialties are relatively well defined, with their patients located on particular wards and with the paediatricians generally not requiring access to the images of the other (adult) patients in the hospital.
Specific advantages of PACS in paediatrics
It is particularly in the NNU/special care baby unit setting that the advantages of PACS are most evident. These mainly premature babies are usually acutely unwell and the changing radiographic findings are often the key factor determining management. As soon as a digital image is acquired onto the PACS it is immediately visible by the clinician on the NNU. Valuable time is saved in not having to go to the Imaging Department to retrieve the image or having to wait for it to be returned to the ward. Patient management decisions can be made immediately at this time, day or night. If a radiologist’s opinion is desired before the formal report is issued, it can be sought by telephone with both paediatrician and radiologist looking at the same image at the same time on different PACS monitors at different locations in the hospital (or at different hospitals or from a home workstation if teleradiology has been implemented).
Once an image has been acquired onto the PACS archive it can never be lost and is always accessible. Even if the image is not on the short term server, it will still be accessible when fetched from the long term archive within minutes, and available for viewing on the ward workstation. In the neonatal and paediatric age range it is even less acceptable than in the adult for a repeat radiograph to be taken simply because the relevant image is missing when needed diagnostically.
On the NNU, or in paediatric patients with chronic diseases, comparative viewing of a sequential series of radiographs/scans is integral to assessment of progress. There are two features of PACS software which facilitate and automate this aspect of medical care: prefetching and default display protocols (DDPs).
PREFETCHING
Prefetching is the process whereby previous images on a patient are automatically retrieved from the long term archive onto the short term server, prior to the acquisition and viewing of the current imaging examination on that patient. This software feature is commonly sufficiently sophisticated to take the form of an “intelligent prefetch”. This means that only a configurable number of examinations from the same modality and of the same body part as that currently being imaged are prefetched from the long term archive; it is usually only these that will be of relevance in making a diagnostic comparison, and there is no point in unnecessarily overloading the PACS network and short term server with data irrelevant to the current clinical problem. Intelligent prefetch software is an advantage of PACS for both paediatric and adult populations. There are many instances where it is highly desirable. Some examples are as follows:
- On the NNU it is helpful to compare the current chest image with previous chest images on the same infant in chronological sequence. It is not useful to have, say, an abdominal or wrist image interspersed among those chest images interrupting the assessment of a progressive change in lung pathology. The same is true when wishing to compare the current abdominal or wrist image with previous images of the same body part.
- In the fracture clinic it is meaningful to compare the current healing tibial fracture with earlier images of the same fracture to assess progress. Suppose the patient also happened to have a fracture of the pelvis two years ago. It would clearly not be meaningful to compare the current appearance of the healing tibial fracture with the last image taken of the healing pelvic fracture. Intelligent prefetch can be set up to recall only the previous tibial images to the short term storage when the patient attends for a follow up tibial radiograph. An ad hoc fetch will always retrieve previous pelvic images from the long term archive, if desired.
Prefetching is triggered by the HIS or the RIS, since it is these computer systems which act as the repository for data such as hospital admissions, outpatient clinic appointments, and the scheduling of further examinations.
DEFAULT DISPLAY PROTOCOLS/HANGING PROTOCOLS
This software feature automatically arranges and displays the current image, with relevant past images on the PACS monitor(s) in the correct chronological order, in a manner which allows immediate comparative viewing without the need for time consuming dragging of images into a preferred configuration. Modern PACS generally allow numerous such DDPs to be personally set up by individual users to cater for individual viewing preferences and for different image types. At Hammersmith a special DDP was designed for viewing neonatal chest images.4 When viewed on a two monitor PACS workstation this automatically paints the current chest image at full resolution on the right hand monitor, and recalls the first image of the current admission to act as the “gold standard” reference, with the five most recent chest images painted as a six on one format on the left hand monitor. A double mouse click on any of these six images renders it full size for more detailed comparison.
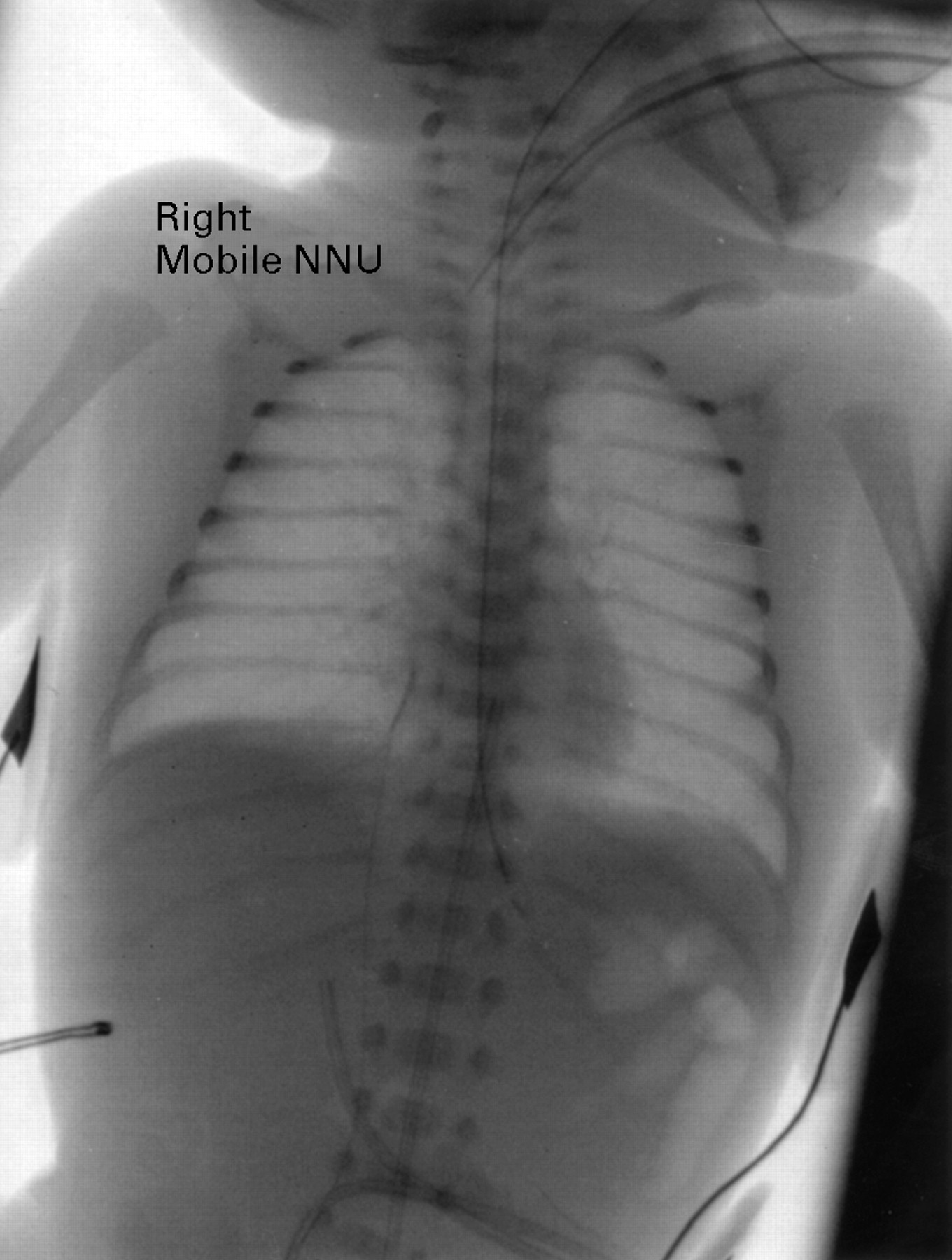
Many of the soft copy post-processing tools available on any PACS workstation (review or diagnostic) are particularly relevant to viewing the paediatric image. Magnification and zoom/pan tools are useful for enlarging and examining in detail the small images of neonates. The “invert greyscale” facility, whereby images may be viewed as black structures on a white background (rather than the conventional white on black presentation) is considered by many to be helpful in precisely identifying the tips of thin lines, such as arterial and venous umbilical catheters (fig 5). The major PACS companies have now perceived the need to provide a means of removing the white area surrounding the exposed image (equivalent to the uncovered area of a conventional light box when viewing a small paediatric radiograph). The small size of paediatric body parts images makes the glare from these white unexposed borders a particular problem in paediatric practice.

{kind=link}
{kind=link}
Figure 5
Inversion of greyscale may be helpful in better visualising tips of thin lines.
The disadvantages of PACS
The installation of a hospital wide PACS is expensive. Even though the price of computer hardware and software has decreased dramatically over the past few years, the cost of implementing a comprehensive PACS in a 500 bed hospital at 1999 prices is still of the order of £1–2 million, with approximately 6% annual maintenance. Studies aimed at assessing the cost benefits of PACS are fraught with practical difficulties,5-7 but a reasonable conclusion is that PACS will pay for itself in about five years after installation from direct and estimated indirect cost savings. There is no question that PACS greatly improves the efficiency of healthcare, although again this is difficult to quantify. It could be argued that it is unreasonable and unrealistic to expect to be able to justify PACS on economic grounds alone, especially as such economic justification is not applied to the installation of new imaging modalities (for example, magnetic resonance or positron emission tomography) also thought to improve healthcare.
When PACS has been installed it is vital to guard against a total system failure as a hospital cannot function without an imaging service. There is no “fall back position” once the hospital has become filmless because the means and infrastructure to generate, distribute, view, and store film no longer exists. As much redundancy as is economically possible needs to be built into the PACS architecture. Daily data backups must occur automatically. Part of the PACS maintenance contract should involve the presence of an information technology engineer on site to deal immediately with day to day problems such as the malfunction of a workstation. A PACS failure, unlike the failure of any other imaging equipment, has such devastating consequences for clinical care that even a minimum delay in resolving the problem is unacceptable. Although many PACS vendors are increasingly relying on remote access modems for maintenance, this is not generally sufficient. A contingency plan should be drawn up in advance to be put into operation should a total system failure occur, so that the hospital is able to maintain a minimal imaging service or emergency work. At Hammersmith Hospital this “PACS failover” mode of operation involves acquiring imaging data locally onto magneto-optical disks (which are later uploaded onto the PACS when it becomes functional again). These data can be viewed on a local workstation. A minimal film printing facility is retained so that images required urgently on the wards can still be printed. Such a contingency plan will need to be implemented in any PACS hospital during major upgrades to the system, which have to be conscientiously planned in advance. The acute nature of NNU clinical care means it is particularly affected by any PACS downtime. Prior to any planned PACS upgrade, the paediatricians (and other acute care clinicians) at Hammersmith are asked to request any vital images on current patients which will be needed for historical comparison during the period when PACS is unavailable, and these are printed on film for temporary use on the wards. Upgrades are instituted during public holidays, when there are no outpatient clinics or routine admissions, in order to minimise disruption to patient care.
Another potential problem of a PACS is the fear that medical staff will not have sufficient computer literacy to be able to use the new technology. This is not an issue for the majority of the current generation of junior doctors. It is important that the graphic user interface of the PACS workstations is as user friendly and intuitive as possible. An increasing number of PACS vendors have realised the benefit of working with clinicians in the design of PACS software to render it clinically relevant and simple to use.8 A minimum amount of initial basic training on the PACS is deemed useful by clinicians, although most appear to learn PACS functionality from their peers.9 A pocket sized instruction card, and online help and/or a computer based training program on the PACS workstations are useful adjuncts.
The future
One of the most significant developments in PACS over the past couple of years has been the exploitation of conventional web browser technology to access images from a short term PACS server and display them on ordinary desktop personal computers. This has provided a cheap and easy means of reviewing images without the need for expensive specialised PACS review workstations. It has also facilitated the development of teleradiology whereby doctors can review emergency images from their homes at night. This would be expected to be a beneficial development if it means that there will be greater recourse to senior medical opinion for difficult emergency cases. Desktop PCs have single colour (relatively low luminance) monitors; there are some areas in the hospital where higher quality two screen diagnostic workstations may still be necessary. These should be located in the radiology department, and probably also in the intensive care units, A&E, and within a communal area accessible to the outpatient consulting rooms.
Now that filmless radiology has been achieved in a number of hospitals worldwide, the next step must be to achieve completely paperless radiology as a step on the way to realising a complete electronic patient record. Paperless radiology requires that there be remote order entry (ROE)/order communications, so that any imaging procedure will be ordered electronically by the requesting physician or general practitioner, directly from the ward, outpatient clinic, or general practice. Generally such electronic requests will be entered onto the hospital information system (HIS), which should be bidirectionally linked to both the radiology information system (RIS) and the PACS. Thus the requesting doctor will have access to the appointments schedule at the time of booking and the clinical details he/she enters will ultimately be transmitted to the PACS to be read in conjunction with the images once these are acquired. It is important that a unique identifier number is generated for each imaging examination, and this number must be known to all computer systems (the RIS, the HIS, and the PACS). This ensures that the appropriate images acquired onto PACS are assigned to the correct examination entry, and are married up with the associated report subsequently dictated. ROE means that the patient no longer has to go to (or contact) the Imaging Department to arrange an appointment and receive a letter containing preprocedural instructions, as both can be generated directly at the computer terminal used for the remote booking. Such an integrated system is much more efficient and avoids the re-entry of textural data at any stage of the clinical workflow, thereby reducing redundancy introduced by human error.
Many see the complete electronic patient record (EPR) as an ultimate goal in both hospital and community practice, although we are still a long way from realising this concept. The EPR would incorporate PACS and ROE, and would contain other clinical data in digital format (histopathology, clinical photographs, electrocardiograms, etc), as well as an electronic version of the patient notes (probably generated by up loading from hand held speech recognition dictation systems used instead of manually writing in the case notes). Some would argue that the EPR should be recorded on a microchip of which a copy is entrusted to the patient. While such a concept may still seem somewhat fanciful, there is no doubt that filmless radiology has already been successfully achieved and that PACS has now proved itself in clinical practice.